
Fetal laser surgery as a last resort
For his dissertation, Joost Akkermans searched for areas of improvement for delicate fetal laser surgery with Twin Transfusion Syndrome (TTS). This syndrome occurs in the Netherlands 60 to 70 times a year among single-egg twins sharing one placenta. Treatment is possible, but not without risk. Inaugural address on 22 June 2017.
Survival not the only criterion
One of Akkermans' propositions in his dissertation states: The long-term follow-up of twins treated in utero is essential to evaluating the success of the treatment, given that the mere survival of the newborn(s) says nothing about their quality of life later in life. In doing so, he wants to point out that the survival of a newborn baby should not be the only criterion for whether to intervene or not: long-term quality of life must also play a role. “It’d later quality of life I think is the most important thing.”
Imbalance in blood exchange
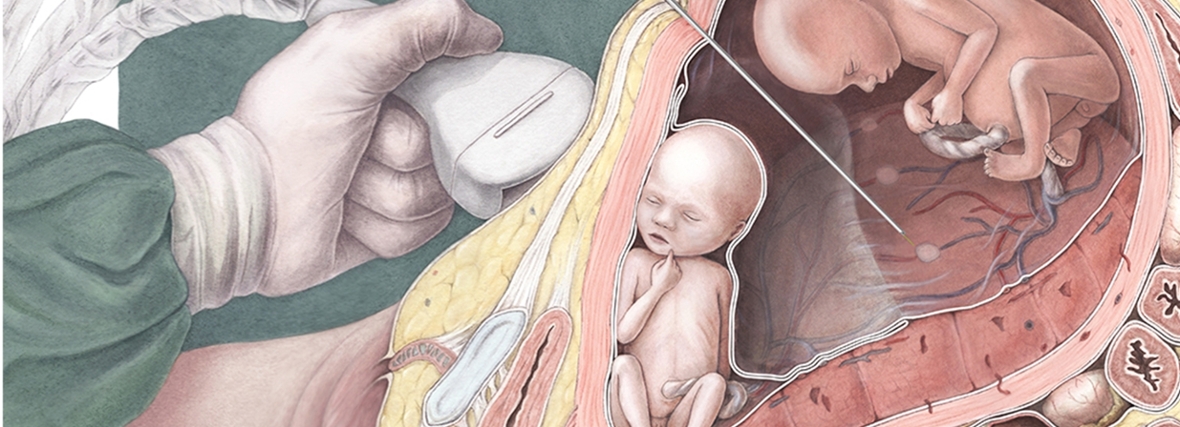
In Twin Transfusion Syndrome (TTS), an imbalance in blood exchange develops between two foetuses in the post-embryonic phase, which the single placenta has to cope with: one foetus receives too much blood, the other too little. Excessive blood puts great stress on the heart, which is forced to pump too hard, and on the kidneys which must process that blood. The foetus must urinate a lot, which quickly expands its amniotic sac. In the other amniotic sac, the opposite occurs: the foetus urinates too little, so that the sac is pulled tighter around the foetus. With no intervention, both foetuses will die.

Small sub-specialism
About 25 years ago, the first milestones were achieved in laser treatment of TTS. Using laser surgery, the arteries in the placenta are cauterised, blocking the exchange of blood between the two foetuses. In this way, they each get their own blood circulation. This is a small, yet relatively new sub-specialism of Gynaecology for which the LUMC is the national expertise centre in the Netherlands. Worldwide, there are around 200 surgeons who conduct this fetal treatment. Akkermans searched for clues for improved treatment and developed a realistic placenta model to evaluate the techniques.
Visible on ultrasound
In 90% of the interventions, at least one foetus survives, in 60 to 70% of cases, both foetuses, which shows that the treatment is not completely without risk. Akkermans: “The danger is that you are too late. We have done much to improve this. TTS can now be seen on ultrasounds, however, it requires a skilled, practised eye. That is why we have devoted a lot of energy in training gynaecologists who do ultrasounds. The protocols for ultrasounds have also been adapted.”
Damage to the placenta
The treatment may cause damage to the placenta itself. In the context of his research, Akkermans, using a test setup (with real placentas), tested what the optimal ratio between the laser wattage and the time required for the treatment. The conclusion: it is better to laser for as short a time as possible with somewhat higher wattage, than vice versa.
Treatment risk
A greater risk is premature birth, which can also be aggravated by the treatment, just as with the chorionic villus sampling test and amniocentesis. Akkermans: “In the case of amniocentesis, and in the treatment of TTS, a needle passes through the membranes. The hole that arises does not fully close. This can result in leakage of amniotic fluid or the membranes can even tear. A 1mm needle is used to make the puncture. This comes with a 1 in 2000 chance that amniotic fluid may leak. In our specialisation, a 3-4mm needle is used, which entails a higher level of risk. Several methods have already been tested to close the gap, including using a plug, but unfortunately a good solution has still to be found.”
Long-term quality of life
According to Akkermans, the link with quality of life is especially strong in premature birth. "The earlier a child is born, the greater the likelihood of constraints in later life, including multiple disabilities. Not long ago, the limit was 32 weeks, but this has already shifted to 24 weeks. I think that in my specialism how these children fare should also be part of the consideration on whether or not to opt for treatment. Hence my position. I have gained inspiration from my colleague Jeanine van Klink, who monitored children for 2 to 4 years who were born after receiving treatment for TTS.”
Akkermans was able to work full-time for two years on his PhD research project, thanks to a grant from the STW Technology Fund. After that, he worked on his research in addition to his specialist training as a gynaecologist.
(CH)